Chronic stress can increase vulnerability to addiction.
Stress is a key risk factor in addiction initiation, maintenance, relapse, and thus treatment failure (Sinha & Jastreboff, 2013). Stressful life events combined with poor coping skills may impact the risk of addiction by increasing impulsive responding and self-medication. While it may not be possible to eliminate stress, we need to find ways to manage it.
Source: Quinn Dombrowski/Wikipedia Commons
Stress normally refers to adversity or hardship such as poverty orgrief. Biologically, stressful events cause a rise in blood levels of stresshormones(such as cortisol). Fight-or-flight is a normal response to stress; all the blood goes to the muscles so that you’re ready for action.
It is important to distinguish between chronic and normal stress. Moderate and challenging stressors with limited duration are perceived as pleasant. In fact, some individuals, like sensation-seekers, chase “stressful” situations that promote the release of stress hormones. However, intense, unpredictable, prolonged stressors,—such as interpersonal conflict, loss of loved ones, and unemployment—can producelearned helplessnessand depressive-like symptoms. Chronic stress increases the risk for developingdepression, the common cold, influenza, tension headaches, grinding teeth, and tensing the neck and shoulders (McEwen, 2003).
Trauma in earlychildhoodis a key factor for making people more vulnerable in later life (Keating, 2017). The link from early adversity to later life problems runs through socialepigenetics. High levels of stress experienced in early life can cause methylation of key genes that control the stress system. That is, early adversity alters ourgenetics. When this happens, we live in a constant state of emergency.
The workplace is another context that provides almost routine exposure to chronic stress.Work-related stressmay include factors such as the demands of the job, the ability to have control over decisions, and the degree of social support within the workplace. People in jobs where they don’t perceive themselves to have a lot of control are susceptible to developing clinicalanxietyand depression, as well as stress-related medical conditions like ulcers and diabetes (Marmot, 2006).
The stressful event or circumstance itself is not harmful. What matters is how the person interprets the stressor and how he or she copes with it. One can use reappraisal as a coping strategy by viewing situations differently, for instance by thinking it's no longer a big deal. One can also cope with stress bysmoking, drinking, and overeating. What is important is the meaning that the event or circumstance has for the individual (Lazarus, 2006).
There is solid evidence for the link between chronic stress and themotivationto use addictive substances (Al'Absi, 2007). For instance, research shows thatadverse childhood experiencessuch as physical and sexual abuse, neglect,domestic violence, and family dysfunction are associated with an increased risk of addiction. People with an unhappymarriage, employment dissatisfaction, or harassment also report increased rates of addiction.
The experience of childhood abuse and neglect indirectly increases the risk of addiction through decreasedself-control(Lovallo, 2013). Young adults at risk forsubstance abuseare known to have decreased self-control and emotional control. Their addictive behavior is the result of their experiences and the environments in which they were brought up.
The greater the number of stressors an individual is exposed to, the greater the later chances of addiction. The economist Angus Deaton (2015) shows that less-educated white Americans who struggle in the job market in early adulthood are likely to experience a “cumulative disadvantage” over time, with health and personal problems that often lead to drug overdoses,alcohol-related liver disease, andsuicide.
One explanation for the strong linkage between stress and addiction is the self-medication theory, which suggests that the person may use drugs to cope with tension associated with life stressors or to relieve symptoms of anxiety and depression resulting from atraumaticevent. Thus, drug use functions as a means to regulate emotions and soothe psychological distress.
High emotional stress is associated with loss of control over impulses and an inability to delay gratification. Chronic stress decreases gray matter volume in the brain region that is associated with cognitive control and stress regulation. The part of the prefrontal cortex that is involved in deliberativecognitionis shut down by stress. The stressed brain loses the ability to be reflective and becomes automatic. Stressed people are prone to give in to impulses like smoking, overeating, alcohol and prescription drug abuse to cope with daily stress (Grant et al., 2011).
In sum, more stressful life events and poor coping strategies may impact risk of addiction. This explains the importance of better understanding how stress works and developing skills to prevent and tolerate it in addiction treatments.
References
Al'Absi Mustafa (2007). Stress and Addiction: Biological and Psychological Mechanisms (2007) Academic press.
Deaton, Angus. (2105), The Great Escape: Health, Wealth, and the Origins of Inequality. Princeton University Press.
Grant, J. E., Donahue, C. B., & Odlaug, B. L. (2011). Overcoming Impulse Control Disorders: A Cognitive - Behavioral Therapy Program (Workbook). New York, NY: Oxford University Press
Keating DP (2017), Born Anxious: The lifelong impact of early life adversity-and how to break the cycle? New york: St Martin Press.
Lazarus R, Lazarus, B (2006) Coping with Aging. New York: Oxford press
Lovallo W. R. (2013). Early life adversity reduces stress reactivity and enhances impulsive behavior: Implications for health behaviors. International Journal of Psychophysiology, 90, 8–16.
Marmot, M. G. (2006). Status syndrome: A challenge to medicine. Journal of the American Medical Association, 295, 1304–1307
McEwen, B. S. (2003). Early life influences on life-long patterns of behavior and health. Mental Retardation and Developmental Disabilities Research Reviews, 9(3), 149-154
Sinha R, Jastreboff AM. Stress as a common risk factor for obesity and addiction. Biol Psychiatry. 2013;73(9):827–835.
You've probably heard of the brain's reward network. It's activated by basic needs — including food, water and sex — and releases a surge of the feel-good neurotransmitter dopamine when those needs are met. But it can also be hijacked by drugs,which lead to a greater dopamine release than those basic needs.
But the reward network isn't the only brain network altered by drug use. A new review concluded that drug addiction affects six main brain networks: the reward, habit, salience, executive, memory and self-directed networks.
In 2016, a total of 20.1 million people ages 12 and older in the U.S. had a substance-use disorder, according to theNational Survey on Drug Use and Health, an annual survey on drug use. And drug addiction, regardless of the substance used, had surprisingly similar effects on the addicted brain, said the new review, published yesterday (June 6) in the journalNeuron.
More than half of the studies out there look at the effects of drug use on the reward network, said Anna Zilverstand, lead author of the new review and an assistant professor of psychiatry at the Icahn School of Medicine at Mount Sinai in New York City. [7 Ways Alcohol Affects Your Health]
"Because we showed that the effects are very distributed across the six different networks … [we can conclude that] an approach that only looks at one of these networks isn't really justified," Zilverstand told Live Science. "This [finding] will hopefully lead other researchers to look beyond the reward network."
For example, the memory network is pretty much ignored in research on substance-use disorders, Zilverstand said. This network allows humans to learn non-habit-based things, such as a new physics concept or a history lesson. Some research has suggested that in people with substance-use disorders, stress shifts the person's learning and memory away from the memory network to the habit network, which drives automatic behavior, such as seeking and taking drugs.
Another less-studied network is the self-directed network, which is involved in self-awareness and self-reflection, the review said. In people with addictions, this network has been associated with increasing craving.
Two other networks are involved insubstance-use disorders: The executive network is normally responsible for goal-maintaining and execution, but drugs can alter this network as well, reducing a person's ability to inhibit their actions. The salience network picks up important cues in a person's environment and redirects the individual's attention to them. (In people with drug addiction, attention is redirected toward drugs, increasing craving and drug-seeking.)
Which comes first, the brain activity or the drug use?
"For me, the most surprising [finding] was how consistent the effects were across addictions," Zilverstand said. What's more, "the fact that the effects are quite independent of the specific drug use points to them being something general that might actually precede drug use rather than be a consequence of drug use."
Zilverstand said she hopes that more studies will look at whether some people have abnormal brain activity in these six networks naturally and if that activity just gets exacerbated if they begin drug use. It's important to knowif some of these traits precede drug use; if that's the case, it might be possible to identify people who are prone to addiction and intervene before an addiction begins, she said.
Some research has pointed toward this possibility already. For example, studies have shown that some people have "difficulties … inhibiting impulsiveness before drug use," Zilverstand said. "Some of these impairments precede drug use, and they may become worse with more drug use, but they exist before the problem escalates."
The good news, however, is that activity in four of these networks — executive, reward, memory and salience — moves back toward "normal" once drug use ends. "We know that four of the networks (partially — not fully) recover but not yet what happens to the other two networks," Zilverstand said in an email.
Zilverstand added that she's particularly excited about an ongoing study called theAdolescent Brain Cognitive Development (ABCD) Study, which is tracking 10,000 children across the U.S. from around ages 9 or 10 to age 20 (the children are now around 13). Some of these individuals will inevitably become addicted to drugs, most likely marijuana or alcohol, Zilverstand said.
"We'll be able to see if the effects that we found [in the review] exist in youth who have not yet abused drugs," she said, and she predicted that researchers will be able to find a lot of the effects identified in the review in the six brain networks.
The authors noted that because some regions of the brain are very small — for example, theamygdala, which is found toward the center of the brain — the studies can't identify strong signals from those areas on brain scans. So, it's possible that drugs affect additional networks in the brain that are hidden because of the limitations of our technologies, Zilverstand said.
"We don't want to conclude that [those effects] don't exist," she said.
Desire initiates the process, but learning sustains it.
The word "addiction" is derived from a Latin term for "enslaved by" or "bound to." Anyone who has struggled to overcome an addiction — or has tried to help someone else to do so — understands why.
Addiction exerts a long and powerful influence on the brain that manifests in three distinct ways: craving for the object of addiction, loss of control over its use, and continuing involvement with it despite adverse consequences. While overcoming addiction is possible, the process is often long, slow, and complicated. It took years for researchers and policymakers to arrive at this understanding.
In the 1930s, when researchers first began to investigate what caused addictive behavior, they believed that people who developed addictions were somehow morally flawed or lacking in willpower. Overcoming addiction, they thought, involved punishing miscreants or, alternately, encouraging them to muster the will to break a habit.
The scientific consensus has changed since then. Today we recognize addiction as a chronic disease that changes both brain structure and function. Just as cardiovascular disease damages the heart and diabetes impairs the pancreas, addiction hijacks the brain. Recovery from addiction involves willpower, certainly, but it is not enough to "just say no" — as the 1980s slogan suggested. Instead, people typically use multiple strategies — including psychotherapy, medication, and self-care — as they try to break the grip of an addiction.
Another shift in thinking about addiction has occurred as well. For many years, experts believed that only alcohol and powerful drugs could cause addiction. Neuroimaging technologies and more recent research, however, have shown that certain pleasurable activities, such as gambling, shopping, and sex, can also co-opt the brain. Although theDiagnostic and Statistical Manual of Mental Disorders, Fourth Edition(DSM-IV) describes multiple addictions, each tied to a specific substance or activity, consensus is emerging that these may represent multiple expressions of a common underlying brain process.
From liking to wanting
Nobody starts out intending to develop an addiction, but many people get caught in its snare. According to the latest government statistics, nearly 23 million Americans — almost one in 10 — are addicted to alcohol or other drugs. More than two-thirds of people with addiction abuse alcohol. The top three drugs causing addiction are marijuana, opioid (narcotic) pain relievers, and cocaine.
Genetic vulnerability contributes to the risk of developing an addiction. Twin and adoption studies show that about 40% to 60% of susceptibility to addiction is hereditary. But behavior plays a key role, especially when it comes to reinforcing a habit.
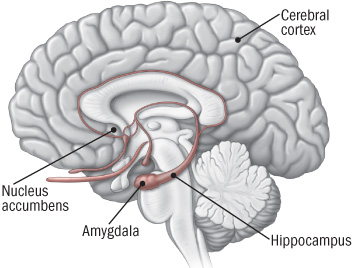
Pleasure principle.The brain registers all pleasures in the same way, whether they originate with a psychoactive drug, a monetary reward, a sexual encounter, or a satisfying meal. In the brain, pleasure has a distinct signature: the release of the neurotransmitter dopamine in the nucleus accumbens, a cluster of nerve cells lying underneath the cerebral cortex (see illustration). Dopamine release in the nucleus accumbens is so consistently tied with pleasure that neuroscientists refer to the region as the brain's pleasure center.
The brain's reward center
Addictive drugs provide a shortcut to the brain's reward system by flooding the nucleus accumbens with dopamine. The hippocampus lays down memories of this rapid sense of satisfaction, and the amygdala creates a conditioned response to certain stimuli.
All drugs of abuse, from nicotine to heroin, cause a particularly powerful surge of dopamine in the nucleus accumbens. The likelihood that the use of a drug or participation in a rewarding activity will lead to addiction is directly linked to the speed with which it promotes dopamine release, the intensity of that release, and the reliability of that release. Even taking the same drug through different methods of administration can influence how likely it is to lead to addiction. Smoking a drug or injecting it intravenously, as opposed to swallowing it as a pill, for example, generally produces a faster, stronger dopamine signal and is more likely to lead to drug misuse.
Learning process.Scientists once believed that the experience of pleasure alone was enough to prompt people to continue seeking an addictive substance or activity. But more recent research suggests that the situation is more complicated. Dopamine not only contributes to the experience of pleasure, but also plays a role in learning and memory — two key elements in the transition from liking something to becoming addicted to it.
According to the current theory about addiction, dopamine interacts with another neurotransmitter, glutamate, to take over the brain's system of reward-related learning. This system has an important role in sustaining life because it links activities needed for human survival (such as eating and sex) with pleasure and reward. The reward circuit in the brain includes areas involved with motivation and memory as well as with pleasure. Addictive substances and behaviors stimulate the same circuit — and then overload it.
Repeated exposure to an addictive substance or behavior causes nerve cells in the nucleus accumbens and the prefrontal cortex (the area of the brain involved in planning and executing tasks) to communicate in a way that coupleslikingsomething withwantingit, in turn driving us to go after it. That is, this process motivates us to take action to seek out the source of pleasure.
Tolerance and compulsion.Over time, the brain adapts in a way that actually makes the sought-after substance or activity less pleasurable.
In nature, rewards usually come only with time and effort. Addictive drugs and behaviors provide a shortcut, flooding the brain with dopamine and other neurotransmitters. Our brains do not have an easy way to withstand the onslaught.
Addictive drugs, for example, can release two to 10 times the amount of dopamine that natural rewards do, and they do it more quickly and more reliably. In a person who becomes addicted, brain receptors become overwhelmed. The brain responds by producing less dopamine or eliminating dopamine receptors — an adaptation similar to turning the volume down on a loudspeaker when noise becomes too loud.
As a result of these adaptations, dopamine has less impact on the brain's reward center. People who develop an addiction typically find that, in time, the desired substance no longer gives them as much pleasure. They have to take more of it to obtain the same dopamine "high" because their brains have adapted — an effect known as tolerance.
At this point, compulsion takes over. The pleasure associated with an addictive drug or behavior subsides — and yet the memory of the desired effect and the need to recreate it (thewanting) persists. It's as though the normal machinery of motivation is no longer functioning.
The learning process mentioned earlier also comes into play. The hippocampus and the amygdala store information about environmental cues associated with the desired substance, so that it can be located again. These memories help create a conditioned response — intense craving — whenever the person encounters those environmental cues.
Cravings contribute not only to addiction but to relapse after a hard-won sobriety. A person addicted to heroin may be in danger of relapse when he sees a hypodermic needle, for example, while another person might start to drink again after seeing a bottle of whiskey. Conditioned learning helps explain why people who develop an addiction risk relapse even after years of abstinence.
Resources
National Clearinghouse for Alcohol and Drug Information P.O. Box 2345 Rockville, MD 20847 800-729-6686 (toll-free) http://ncadi.samhsa.gov
National Institute on Alcohol Abuse and Alcoholism 5635 Fishers Lane, MSC 9304 Bethesda, MD 20892 301-443-3860 www.niaaa.nih.gov
National Institute on Drug Abuse 6001 Executive Blvd., Room 5213 Bethesda, MD 20892 301-443-1124 www.nida.nih.gov
Substance Abuse and Mental Health Services Administration 1 Choke Cherry Road Rockville, MD 20857 877-276-4727 (toll-free) www.samhsa.gov
The long road to recovery
Because addiction is learned and stored in the brain as memory, recovery is a slow and hesitant process in which the influence of those memories diminishes.
About 40% to 60% of people with a drug addiction experience at least one relapse after an initial recovery. While this may seem discouraging, the relapse rate is similar to that in other chronic diseases, such as high blood pressure and asthma, where 50% to 70% of people each year experience a recurrence of symptoms significant enough to require medical intervention.
Fortunately a number of effective treatments exist for addiction, usually combining self-help strategies, psychotherapy, and rehabilitation. For some types of addictions, medication may also help.
The precise plan varies based on the nature of the addiction, but all treatments are aimed at helping people to unlearn their addictions while adopting healthier coping strategies — truly a brain-based recovery program.
Benowitz NL. "Nicotine Addiction,"The New England Journal of Medicine(June 17, 2010): Vol. 362, No. 24, pp. 2295–303.
Brady KT, et al., eds.Women and Addiction: A Comprehensive Handbook(The Guilford Press, 2009).
Chandler RK, et al. "Treating Drug Abuse and Addiction in the Criminal Justice System: Improving Public Health and Safety,"Journal of the American Medical Association(Jan. 14, 2009): Vol. 301, No. 2, pp. 183–90.
Greenfield SF, et al. "Substance Abuse Treatment Entry, Retention, and Outcome in Women: A Review of the Literature,"Drug and Alcohol Dependence(Jan. 5, 2007): Vol. 86, No. 1, pp. 1–21.
Koob GF, et al. "Neurocircuitry of Addiction,"Neuropsychopharmacology(Jan. 2010): Vol. 35, No. 1, pp. 217–38.
McLellan AT, et al. "Drug Dependence, A Chronic Medical Illness: Implications for Treatment, Insurance, and Outcomes Evaluation,"Journal of the American Medical Association(Oct. 4, 2000): Vol. 284, No. 13, pp. 1689–95.
National Institute on Drug Abuse.Drugs, Brains, and Behavior: The Science of Addiction(National Institutes of Health, Aug. 2010).
Polosa R, et al. "Treatment of Nicotine Addiction: Present Therapeutic Options and Pipeline Developments,"Trends in Pharmacological Sciences(Jan. 20, 2011): E-publication.
Potenza MN, et al. "Neuroscience of Behavioral and Pharmacological Treatments for Addictions,"Neuron(Feb. 24, 2011): Vol. 69, No. 4, pp. 695–712.
Shaffer HJ, et al. "Toward a Syndrome Model of Addiction: Multiple Expressions, Common Etiology,"Harvard Review of Psychiatry(Nov.–Dec. 2004): Vol. 12, No. 6, pp. 367–74. *
Stead LF, et al. "Nicotine Replacement Therapy for Smoking Cessation,"Cochrane Database of Systematic Reviews(Jan. 23, 2008): Doc. No. CD000146.
Substance Abuse and Mental Health Services Administration.National Survey on Drug Use & Health, 2009.